| |
16:30
|
0197.
 |
Rapid Device Localization for Prospective Stereotaxy: Using
Computation Instead of Imaging - Permission Withheld
Miles E. Olsen1, Ethan K. Brodsky1,
Jonathan A. Oler2, Marissa K. Riedel2,
Eva M. Fekete2, Ned H. Kalin2, and
Walter F. Block1
1Medical Physics, University of Wisconsin -
Madison, Madison, WI, United States, 2Psychiatry,
University of Wisconsin - Madison, Madison, WI, United
States
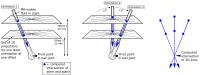
We present a technique for rapidly aiming interventional
devices during prospective stereotaxy procedures. Our
approach enables accurate computational determination of
trajectory guide orientation and the true physical pivot
point of frameless stereotaxy guides that mount on the
skull.
Historically, these neurosurgical tasks require minutes
per iterative cycle consisting of: scan, interpret image,
adjust aim, repeat – or no intraoperative imaging at all,
relying on preoperative images registered to stereotactic
frame coordinates. Our rapid technique (~5 FPS) is closer to
the clinician’s preferred responsiveness of optical tracking
of devices in the OR (~30 FPS).
|
| |
16:42
|
0198.
 |
Evaluation of Infection Risk for MR Guided DBS Implantations in
a Radiology Suite 
Alastair Martin1, Paul Larson2, Nadja
Levesque2, Jill Ostrem3, and Philip
Starr2
1Radiology and Biomedical Imaging, UCSF, San
Francisco, CA, United States, 2Neurological
Surgery, UCSF, San Francisco, CA, United States, 3Neurology,
UCSF, San Francisco, CA, United States
Hardware infection incidence for DBS implantations performed
in a diagnostic MR suite is reported. A total of 164 DBS
procedures were performed in movement disorder patients
resulting in six (3.7%) hardware related infections. Two
infections occurred within the first 10 cases and led to a
change in sterile practice. Over the last 154 cases four
(2.6%) infections have been reported and all were associated
with implantation of the IPG controller, which is done in a
separate surgical procedure 1-3 weeks after DBS
implantation. Infection risk when implanting DBS electrodes
in a diagnostic MR suite is comparable to conventional OR
procedures.
|
| |
16:54
|
0199.
 |
Time-resolved 23-Na Imaging for Monitoring of Thermochemical
Ablation Injections
Nicolas G.R. Behl1, Armin M. Nagel1,2,
Erik N.K. Cressman3, Reiner Umathum1,
David Fuentes4, R. Jason Stafford4,
Peter Bachert1, Mark E. Ladd1, and
Florian Maier1
1Medical Physics in Radiology, German Cancer
Research Center (DKFZ), Heidelberg, Germany, 2Diagnostic
and Interventional Radiology, University Medical Center Ulm,
Ulm, Germany, 3Interventional
Radiology, M. D. Anderson Cancer Center, Houston, TX, United
States, 4Imaging
Physics, M. D. Anderson Cancer Center, Houston, TX, United
States
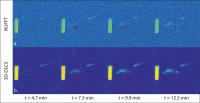
Thermochemical ablation (TCA) is a novel minimally invasive
ablation approach. Acetic acid and sodium hydroxide are
injected simultaneously and mix and react directly before
entering the tissue. The exothermal reaction releases heat
that is used for thermal ablation. For a detailed
characterization of TCA injection, 4D 23Na-data
with reasonable temporal resolution are required. In this
work, a compressed sensing approach was applied to acquire
4D 23Na-data
of injections with high spatial and good temporal
resolution.
|
| |
17:06
 |
0200.
 |
Intrinsic MR visualization of RF lesions using IR-SSFP after
MR-guided ablation
Philippa Krahn1,2, Venkat Ramanan2,
Labonny Biswas2, Nicolas Yak2, Kevan
Anderson2, Jennifer Barry2, Sheldon
Singh3, Mihaela Pop1,2, and Graham A
Wright1,2
1Medical Biophysics, University of Toronto,
Toronto, ON, Canada, 2Physical
Sciences, Sunnybrook Research Institute, Toronto, ON,
Canada, 3Cardiology,
Sunnybrook Health Sciences Centre, Toronto, ON, Canada
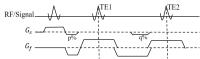
Here we explored an efficient imaging protocol for
visualizing both the edema (reversible) and necrosis
(irreversible) regions of myocardial injury in RF lesions.
Using an MR-guided catheter system, we performed ablation in
swine, immediately followed by T1-based imaging
(IR-SSFP) and T2 mapping
(T2-prepared SSFP) for lesion characterization.
The areas of edema segmented from IR-SSFP images and T2maps
were visually similar and showed good correlation. IR-SSFP
is known to visualize lesion cores at a specific
TI--selecting an additional TI which emphasizes edema, we
successfully demonstrated that both regions could be
visualized by a single IR-SSFP acquisition.
|
| |
17:18
 |
0201.
 |
In-vivo echo-navigated MR thermometry for real-time monitoring
of cardiac radiofrequency ablation
Solenn Toupin1,2, Matthieu Lepetit-Coiffe2,
Pierre Bour1, Valery Ozenne1, Baudouin
Denis de Senneville3, Rainer Schneider4,
Kimble Jenkins5, Arnaud Chaumeil1,
Pierre Jais1, and Bruno Quesson1
1IHU-LIRYC, Bordeaux, France, 2Siemens
Healthcare, Saint Denis, France, 3Mathematical
Institute of Bordeaux, Bordeaux, France, 4Siemens
Healthcare, Erlangen, Germany, 5MRI
Interventions, Irvine, CA, United States
The visualization of lesion formation in real time is one
potential benefit of carrying out radiofrequency ablation
(RFA) under magnetic resonance (MR) guidance in the
treatment of ventricular arrhythmia. In this study, we
propose a real-time MR thermometry method to visualize
online the temperature distribution in the myocardium during
catheter-based RFA. An echo-navigated sequence is used with
slice tracking to compensate respiratory-induced
through-plane motion and allow all image orientation. The
method was evaluated during free breathing in 5 healthy
volunteers and during RF delivery on the left ventricle (LV)
of a sheep in vivo.
|
| |
17:30
|
0202.
 |
GPU Accelerated Dynamic Respiratory Motion Model Correction for
MRI-Guided Cardiac Interventions
Robert Xu1,2 and
Graham Wright1,2
1Medical Biophysics, University of Toronto,
Toronto, ON, Canada, 2Schulich
Heart Research Program, Sunnybrook Research Institute,
Toronto, ON, Canada
The objective of this study is to explore the use of a
rapidly updated dynamic motion model to correct for
respiratory motion induced errors during MRI-guided cardiac
interventions. The motivation for the proposed technique is
to improve the accuracy of MRI guidance by taking advantage
of the anatomical context provided by the high-resolution
prior images and the respiratory motion information present
in a series of real-time MR images. To achieve this goal,
the proposed dynamic motion model is updated continuously,
and is used to predict the motion estimate for realigning
the prior volume with the real-time images during an
intervention.
|
| |
17:42
|
0203.
 |
An MR-compatible Assistance System for MR-guided Needle
Interventions: Initial Phantom Evaluation
Axel Joachim Krafft1,2,3, Simon Reiss2,
Andreas Reichert2, Michael Vogele4,
and Michael Bock2
1German Cancer Consortium (DKTK), Heidelberg,
Germany, 2Radiology
– Medical Physics, University Medical Center Freiburg,
Freiburg, Germany, 3German
Cancer Research Center (DKFZ), Heidelberg, Germany,4iSYS
Medizintechnik GmbH, Kitzbuehel, Austria
Minimally invasive interventions highly benefit from imaging
guidance during instrument positioning and monitoring of
therapeutic progress. MRI with its unique soft tissue
contrast and ability for functional imaging is ideally
suited for interventional guidance. To enable and facilitate
minimally invasive interventions in closed-bore high-field
MR systems with small bore diameters that severely limit
patient access, we propose a novel, versatile assistance
system in combination with passive instrument tracking. The
system was studied in a systematic phantom experiment during
needle procedures, and a mean targeting accuracy of less
than 2 mm was achieved (mean procedure time: 6.5 min).
|
| |
17:54
|
0204.
 |
Dual echo z-shimmed sequence for PRF-shift MR thermometry near
metallic ablation probes
Yuxin Zhang1 and
William A Grissom2
1Biomedical Engineering, Tsinghua University,
Beijing, China, People's Republic of, 2Biomedical
Engineering, Vanderbilt University Institute of Imaging
Science, Nashville, TN, United States
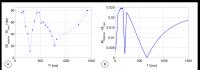
Signal loss induced by ablation probe prevents accurate
temperature monitoring where the thermal dose is highest. To
address this problem, a dual echo sequence with z-shimming
is proposed to recover the signal and an associated
penalized likelihood approach is applied to estimate a
single temperature map from both echoes. Phantom experiments
were conducted to validate the effect of the proposed
sequence. Evident signal recovery is shown in the magnitude
images and temperature maps with heating. Standard deviation
maps with no heating are presented to reflect the large
reduction in uncertainty over time with dual-echo z-shimmed
thermometry.
|
| |
18:06
|
0205.
 |
In vivo monitoring of percutaneous thermal ablation by
simultaneous MR Elastography and Thermometry
Nadège Corbin1, Jonathan Vappou1,
Pramod Rao1, Benoit Wach1, Laurent
Barbé1, Pierre Renaud1, Michel de
Mathelin1, and Elodie Breton1
1ICube-University of Strasbourg, Strasbourg,
France
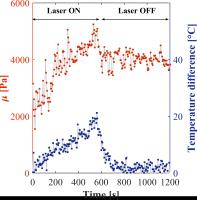
MR-guided percutaneous thermal ablations are currently
monitored by MR thermometry. However, no information related
to intrinsic property changes of the tissue is available
during the procedure. The feasibility of monitoring in vivo
thermal ablations by simultaneous Magnetic Resonance
Elastography (MRE) and MR-thermometry is demonstrated in
this work. The interventional MRE system includes a needle
MRE driver, a respiratory triggered gradient-echo sequence
with motion encoding and an online reconstruction method
that provides elasticity and temperature measurements in
real-time. Changes in elasticity and temperature occurring
during laser thermal ablation are successfully measured in
vivo over 20 minutes thanks to this interventional MRE
system.
|
| |
18:18
|
0206.
 |
Preliminary evaluation of R2*-based temperature mapping for
predicting the kill zone in MRI-guided renal cryoablation
Junichi Tokuda1, Kemal Tuncali1,
Lisanne Kok1,2, Vincent M Levesque 1,
Ravi T Seethamraju 3,
Clare M Tempany1, and Ehud J Schmidt1
1Department of Radiology, Brigham and Women's
Hospital, Boston, MA, United States, 2Eindhoven
University of Technology, Eindhoven, Netherlands, 3Siemens
Healthcare, Boston, MA, United States
We tested the feasibility of R2*-based temperature mapping
using a PETRA UTE sequence to determine the “kill zone”
within an ice ball in the kidney during MRI-guided renal
cryoablation. R2*-maps were calculated from dual-echo PETRA
images acquired during six renal cryoablation cases, and
converted to temperature maps using R2*-temperature
calibrations performed in swine kidneys. We compared
ablation volumes estimated from (a) the -20°C boundary on
the temperature maps; (b) the signal void on
intra-procedural T2-weighted images; and (c) post-ablation
contrast-enhanced MRI as the “gold standard”. Results show
that R2*-based temperature maps provided a reliable lower
limit of the kill-zone volume.
|
|