Shuo Zhang1, Janine Knapp2, Roland Cronenberg3, Björn Schönnagel2, Manuela Tavares de Sousa4, Barbara Ulm5, Daniela Prayer3, Vanessa Berger-Kulemann3, and Fabian Kording2,6
1Philips, Hamburg, Germany, 2Department of Diagnostic and Interventional Radiology and Nuclear Medicine, University Hospital Hamburg-Eppendorf, Hamburg, Germany, 3Department of Biomedical Imaging and Image-Guided Therapy, Division of Neuroradiology and Musculoskeletal Radiology, Medical University of Vienna, Vienna, Austria, 4Department of Obstetrics and Fetal Medicine, University Hospital Hamburg-Eppendorf, Hamburg, Germany, 5Department of Gynecology and Obstetrics, Division of Feto-Maternal Medicine, Medical University of Vienna, Vienna, Austria, 6northh medical GmbH, Hamburg, Germany
1Philips, Hamburg, Germany, 2Department of Diagnostic and Interventional Radiology and Nuclear Medicine, University Hospital Hamburg-Eppendorf, Hamburg, Germany, 3Department of Biomedical Imaging and Image-Guided Therapy, Division of Neuroradiology and Musculoskeletal Radiology, Medical University of Vienna, Vienna, Austria, 4Department of Obstetrics and Fetal Medicine, University Hospital Hamburg-Eppendorf, Hamburg, Germany, 5Department of Gynecology and Obstetrics, Division of Feto-Maternal Medicine, Medical University of Vienna, Vienna, Austria, 6northh medical GmbH, Hamburg, Germany
Fetal cardiovascular MRI was
possible with direct fetal cardiac gating by the DUS device. Benefits were shown
with promise in high-quality morphological and functional studies of the fetal heart
using routinely available imaging techniques, including cine, 4D flow and myocardial
mapping.
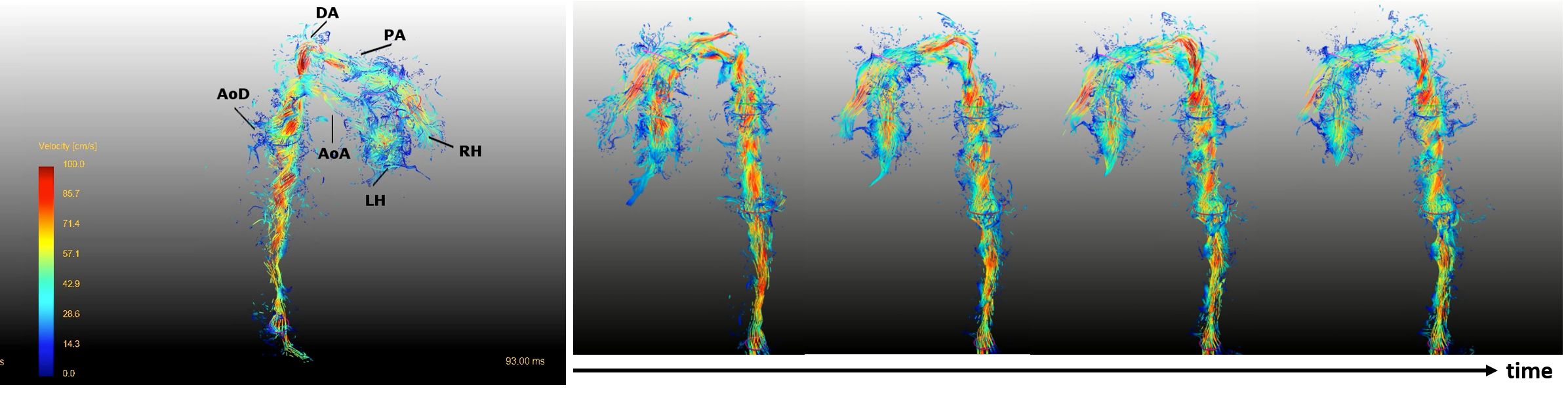
Figure 3. 4D flow exam of the fetal heart based on DUS fetal cardiac gating. Image examples with streamline visualization were selected from a case at 35 gestational weeks on 3.0T. Details see text.
DA = ductus arteriosus; PA = pulmonary artery; AoD = descending aorta; AoA = ascending aorta; RH = right heart; LH = left heart
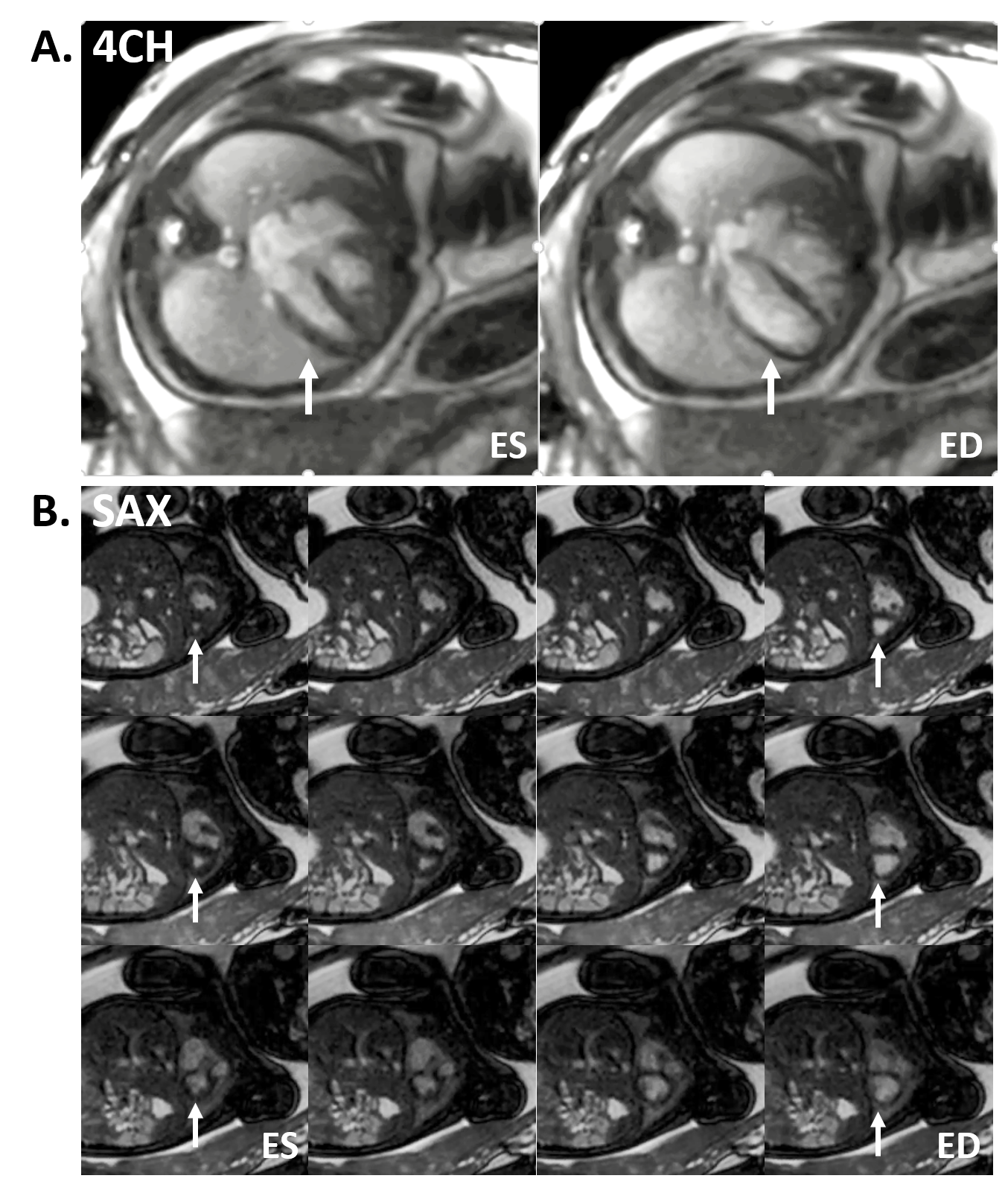
Figure 2. Functional cine exams of the fetal
heart based on DUS fetal cardiac gating on 3.0T. (A) Selected images in 4-chamber view (4CH) at end
systole (ES) and end diastole (ED). (B) Selected images from three
adjacent short-axis slices (SAX) from ES to ED. Arrows indicated the fetal
heart at ES and ED.
