Ehsan Kazemivalipour1,2,3, Alireza Sadeghi-Tarakameh4, Boris Keil5, Yiğitcan Eryaman4, Ergin Atalar1,2, and Laleh Golestanirad3,6
1Electrical and Electronics Engineering Department, Bilkent University, Ankara, Turkey, 2National Magnetic Resonance Research Center (UMRAM), Bilkent University, Ankara, Turkey, 3Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 4Center for Magnetic Resonance Research (CMRR), University of Minnesota, Minneapolis, MN, United States, 5Institute of Medical Physics and Radiation Protection, Mittelhessen University of Applied Sciences, Giessen, Germany, 6Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, Evanston, IL, United States
1Electrical and Electronics Engineering Department, Bilkent University, Ankara, Turkey, 2National Magnetic Resonance Research Center (UMRAM), Bilkent University, Ankara, Turkey, 3Department of Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 4Center for Magnetic Resonance Research (CMRR), University of Minnesota, Minneapolis, MN, United States, 5Institute of Medical Physics and Radiation Protection, Mittelhessen University of Applied Sciences, Giessen, Germany, 6Department of Biomedical Engineering, McCormick School of Engineering, Northwestern University, Evanston, IL, United States
Performing MRI at higher static fields is not necessarily more dangerous than lower fields in patients with conductive implants. When global SAR is set as the upper limit, coils at higher resonance frequency generate less local SAR due to decreased B1+ levels.
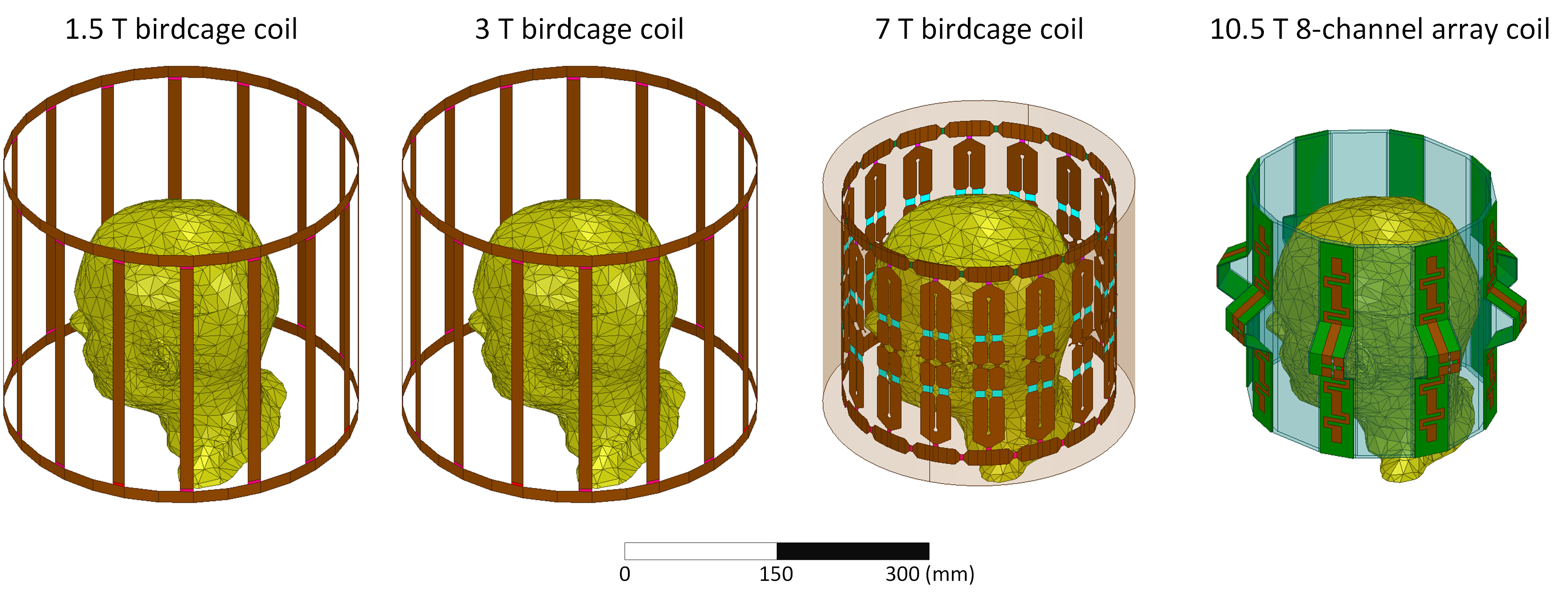
Figure 1 – Numerical models of a 1.5 T 16-rung low-pass birdcage coil tuned at 64 MHz, a 3 T 16-rung low-pass birdcage coil tuned at 127 MHz, a 7 T 16-rung hybrid birdcage coil tuned at 297 MHz, and a 10.5 T 8-channel bumped dipole coil tuned at 447 MHz all loaded with a uniform human head model with no implant. The geometrical dimensions of the coils were the same as the coils reported in the literature2-5.
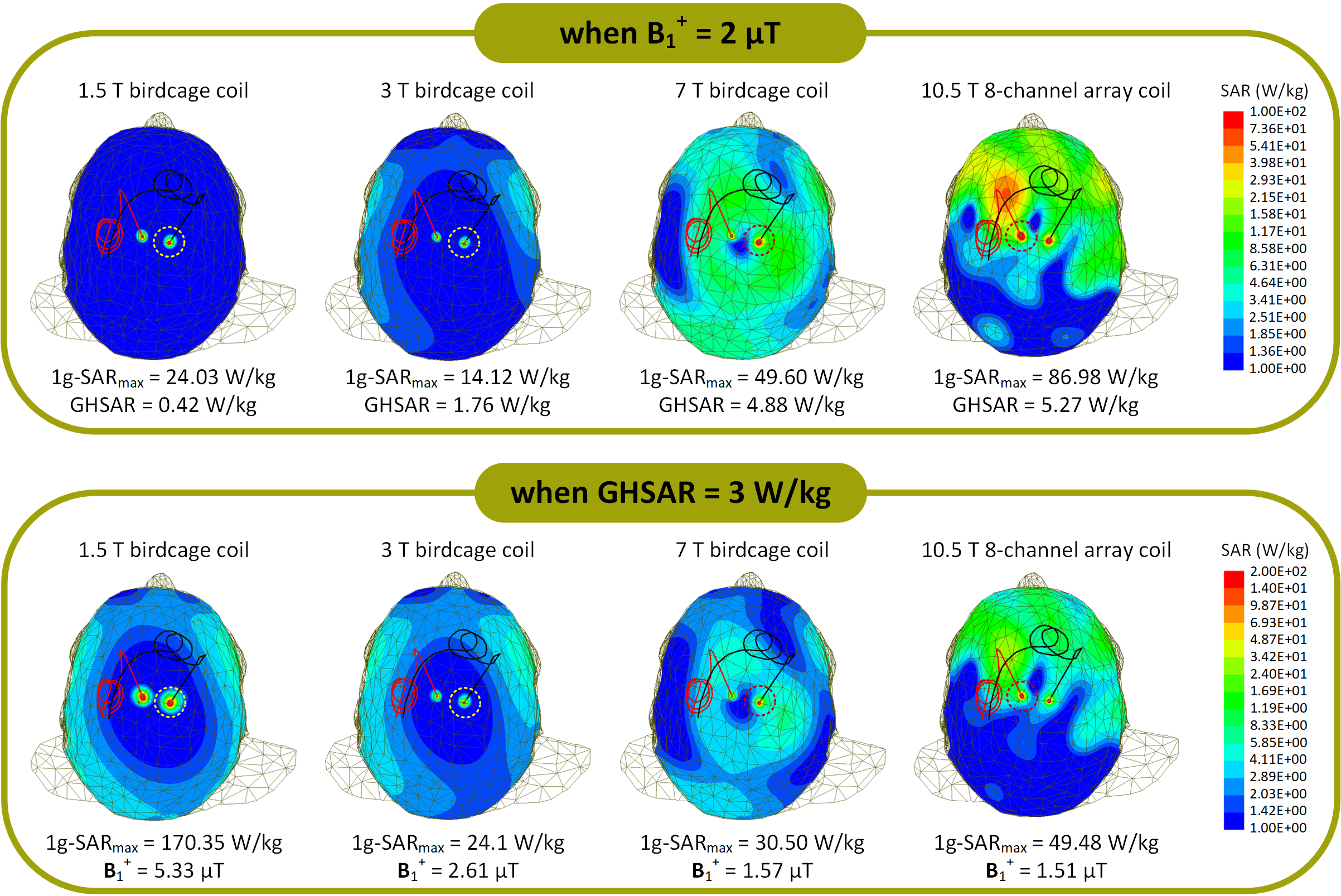
Figure 3 - 1g-SAR distributions in patient 10 (ID10) for the 1.5 T, 3 T, 7 T, and 10.5 T coils on an axial plane passing through the electrode contacts. The coils' input powers were adjusted (A) to generate an average of B1+ = 2 μT and (B) to produce a GHSAR = 3 W/kg over an axial plane passing through the patient's eyes.