Joshua S Greer1,2,3, Mubeena Abdulkarim1, Gerald F Greil1,3, Ayesha Zia1, Ananth J Madhuranthakam2,3, and Tarique Hussain1,2
1Pediatrics, UT Southwestern Medical Center, Dallas, TX, United States, 2Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 3Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States
1Pediatrics, UT Southwestern Medical Center, Dallas, TX, United States, 2Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 3Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States
Perfusion imaging using ASL was
demonstrated in pediatric patients with pulmonary embolism, which successfully
detected perfusion defects in all patients. A method to quantify pulmonary
vascular obstruction was developed using ASL, which showed moderate agreement
with CT angiography.
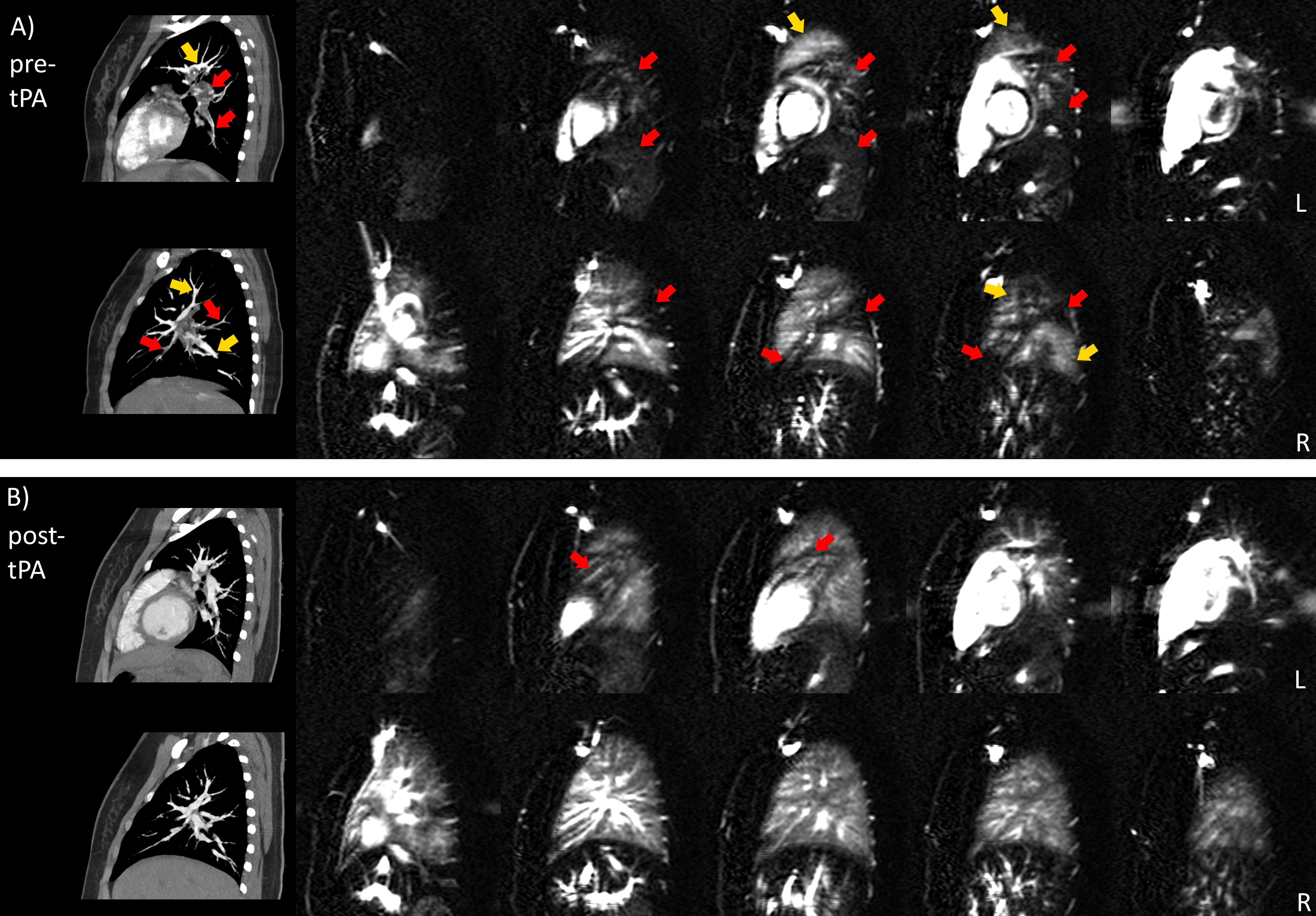
Figure 3: (A) MS-FAIR perfusion and
CTA images in a patient with extensive PE at diagnosis. Red arrows show CTA pulmonary
artery filling defects, which correspond well with ASL perfusion defects.
Yellow arrows indicate vessels with normal filling on CT that correspond well
with regions of higher ASL perfusion.
(B) The same patient 6 months after tPA treatment, showing
significantly improved perfusion. PVO before and after treatment were 73% and 8%
measured by CT, and 63% and 39% by ASL. A residual defect was detected by ASL (B,
red arrows), while the vascular occlusion by CT had resolved.
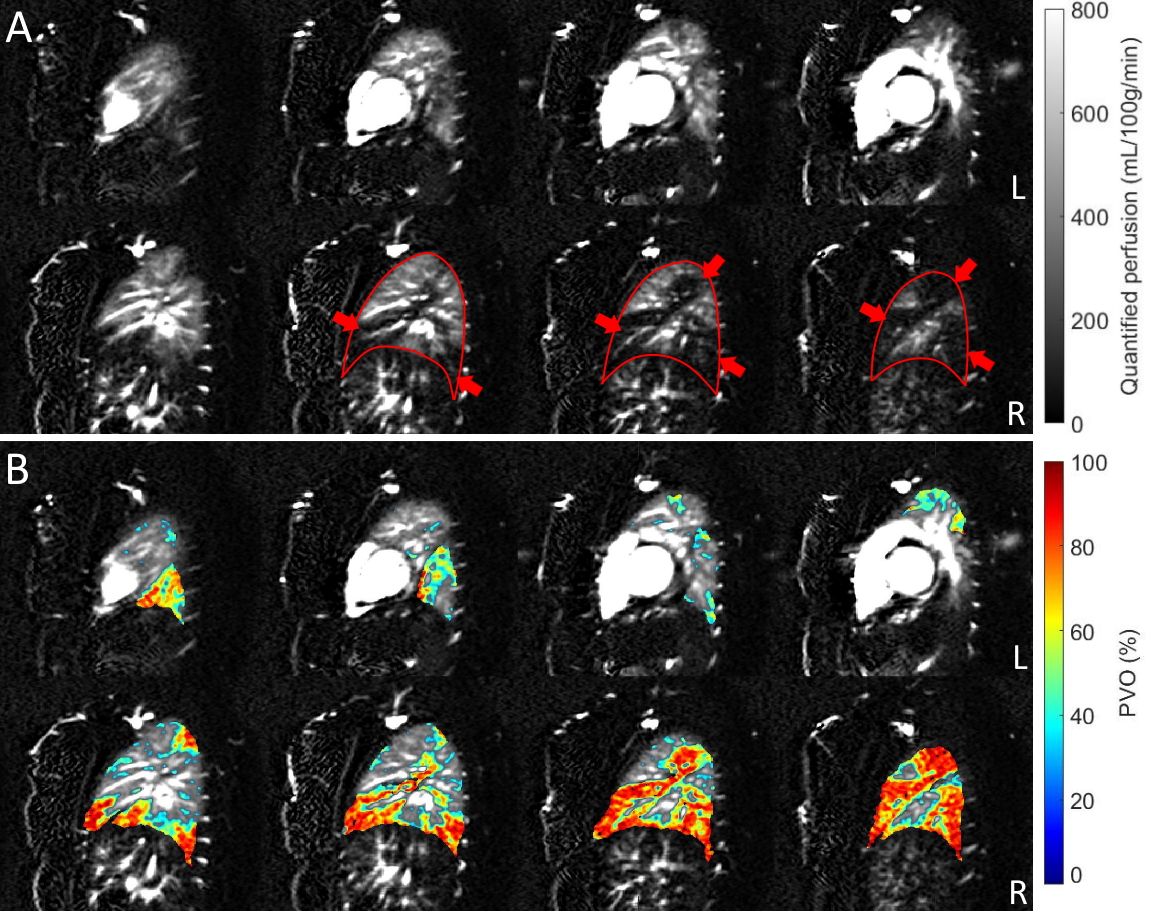
Figure 1: (A) Sagittal MS-FAIR quantified perfusion images
in a patient with extensive filling defects across the right lung noted by CTA
6 days prior to ASL imaging. The edges of the right lung are outlined in red.
Average PVO for this patient was 55% measured by CTA, and 44% measured by ASL.
(B) Overlaid PVO values on the perfusion images, with higher
degrees of obstruction corresponding well with the perfusion defects in Fig 1A.
Overlaid PVO values under 50% were made transparent for visualization purposes
