Michelle Pryde1,2, Sarah Reeve2,3, Taylor Bouchie2,4, Elena Adela Cora5,6, David Volders5,6, Chris Bowen2,3,5, James Rioux2,3,5, and Steven Beyea1,2,3,5
1School of Biomedical Engineering, Dalhousie University, Halifax, NS, Canada, 2Biomedical Translational Imaging Centre, QEII Health Sciences Centre, Halifax, NS, Canada, 3Physics and Atmospheric Science, Dalhousie University, Halifax, NS, Canada, 4Medicine, Dalhousie University, Halifax, NS, Canada, 5Diagnostic Radiology, Dalhousie University, Halifax, NS, Canada, 6Diagnostic Imaging, Nova Scotia Health, Halifax, NS, Canada
1School of Biomedical Engineering, Dalhousie University, Halifax, NS, Canada, 2Biomedical Translational Imaging Centre, QEII Health Sciences Centre, Halifax, NS, Canada, 3Physics and Atmospheric Science, Dalhousie University, Halifax, NS, Canada, 4Medicine, Dalhousie University, Halifax, NS, Canada, 5Diagnostic Radiology, Dalhousie University, Halifax, NS, Canada, 6Diagnostic Imaging, Nova Scotia Health, Halifax, NS, Canada
On a low-field, point-of-care MRI system, radiologists' confidence in identifying clinical features necessary to triage acute stroke (i.e. DWI-T2 FLAIR mismatch) remains high despite retrospective acceleration of up to R=6.
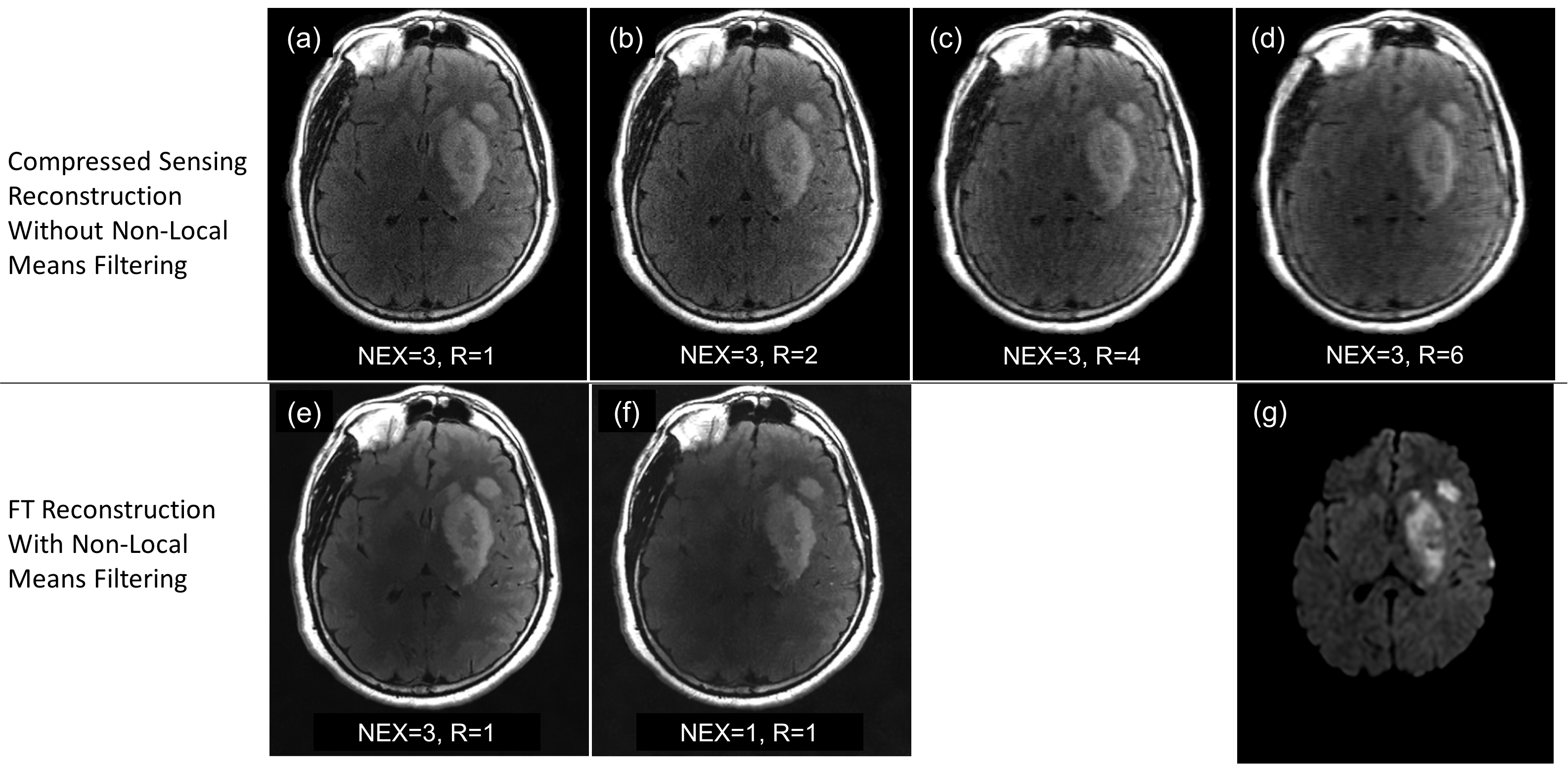
Images (a)-(d) and (e)-(f) demonstrate T2 FLAIR images
processed with
two different pipelines so as to independently explore their effects on
radiologists’ confidence scores. Image
(g) is the corresponding native
DWI. The stroke pictured is that
for which radiologists’ confidence averaged over all DWI-T2 FLAIR pairs
was highest when
answering questions related to
acute stroke; average scores for presence of
acute infarct, location of acute infarct,
and DWI-T2 FLAIR mismatch were
5.0, 5.0, and 4.3, respectively.
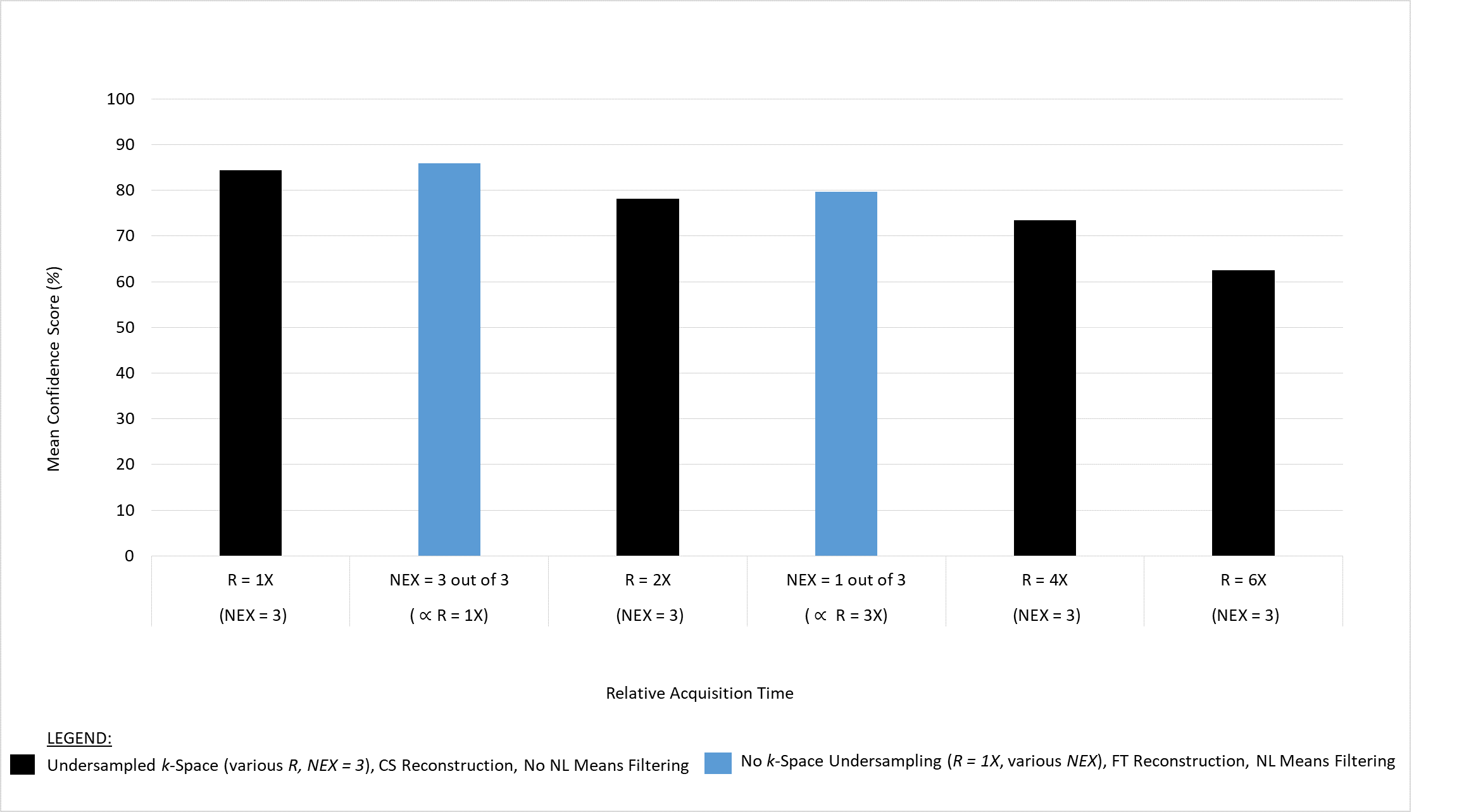
Mean radiologist confidence score in identification of DWI-T2 FLAIR mismatch for acute ischemic stroke versus relative acquisition time. The data illustrate that reducing relative acquisition time by up to R=6 yields a decrease in radiologists' confidence in the accuracy of their identification of DWI-T2 FLAIR mismatch, at most, by 23%.
