Alexandros Patsanis1, Mohammed R. S. Sunoqrot 1, Elise Sandsmark 2, Sverre Langørgen 2, Helena Bertilsson 3,4, Kirsten M. Selnæs 1,2, Hao Wang5, Tone F. Bathen 1,2, and Mattijs Elschot 1,2
1Department of Circulation and Medical Imaging, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 2Department of Radiology and Nuclear Medicine, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway, 3Department of Clinical and Molecular Medicine, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 4Department of Urology, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway, 5Department of Computer Science, Norwegian University of Science and Technology - NTNU, Gjøvik, Norway
1Department of Circulation and Medical Imaging, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 2Department of Radiology and Nuclear Medicine, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway, 3Department of Clinical and Molecular Medicine, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 4Department of Urology, St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway, 5Department of Computer Science, Norwegian University of Science and Technology - NTNU, Gjøvik, Norway
Weakly-supervised GANs trained on
normalized, randomly sampled images of size 128x128 with a 0.5 mm pixel spacing
gave the best AUC for detection of prostate cancer on T2-weighted MR images.
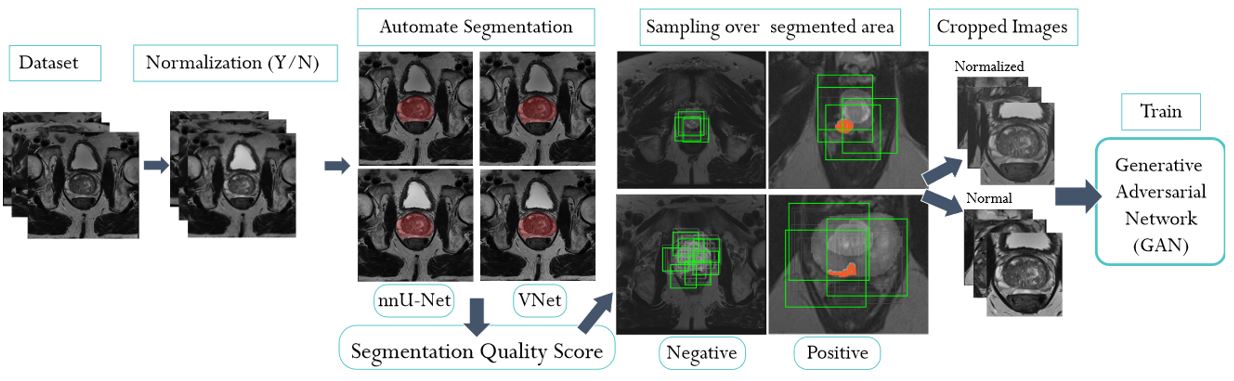
Figure 1: The
proposed end-to-end pipeline includes automated
intensity normalization using AutoRef5, automated prostate
segmentation using VNet6 and nnU-Net7 followed by an
automated Quality Control step, and the sampling of cropped images with
different techniques and settings. The cropped images were then used to train weakly-supervised (Fixed-Point GAN)
and unsupervised GAN (f-AnoGAN) models.
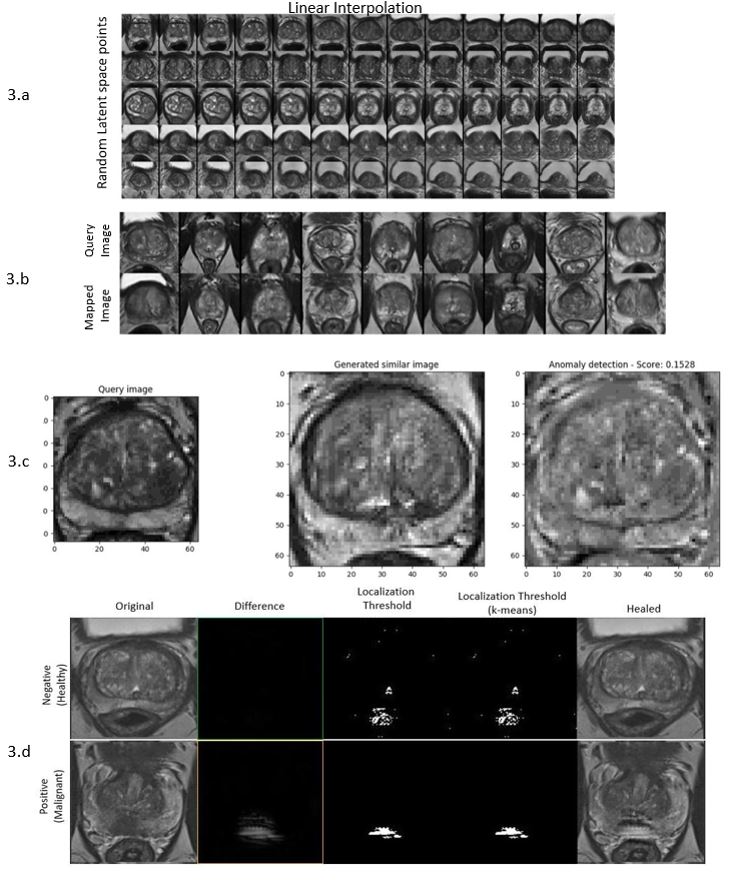
Figure 3: f-AnoGAN and Fixed-Point
GAN - 3.a) f-AnoGAN: Linear latent space interpolation for random endpoints of
trained f-AnoGAN shows that the model does not focus only on one part of the
training dataset. 3.b) f-AnoGAN: Mapping
from image space (query) back to GAN's latent space should yield resembled
images. Here, the mapped images are similar but not entirely identical. 3.c) f-AnoGAN:
Positive test case that fails– 3.d) Fixed-Point GAN: negative and positive tested cases, no
differences for the negative case, whereas positive case found, and localized (difference).
