Li Jiang1,2, Brenda Hanna-Pladdy1,2, Jiachen Zhuo1,2, Paul Fishman3, and Rao Gullapalli1,2
1Center for Advanced Imaging Research, University of Maryland Baltimore, Baltimore, MD, United States, 2Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland Baltimore, Baltimore, MD, United States, 3Department of Neurology, University of Maryland Baltimore, Baltimore, MD, United States
1Center for Advanced Imaging Research, University of Maryland Baltimore, Baltimore, MD, United States, 2Department of Diagnostic Radiology & Nuclear Medicine, University of Maryland Baltimore, Baltimore, MD, United States, 3Department of Neurology, University of Maryland Baltimore, Baltimore, MD, United States
Our findings showed that multimodal disruption of cerebellar connectivity while reflective of early symptoms of PD, also may suggest a possible compensatory mechanism prior to clinical presentation of non-motor features of the disease.
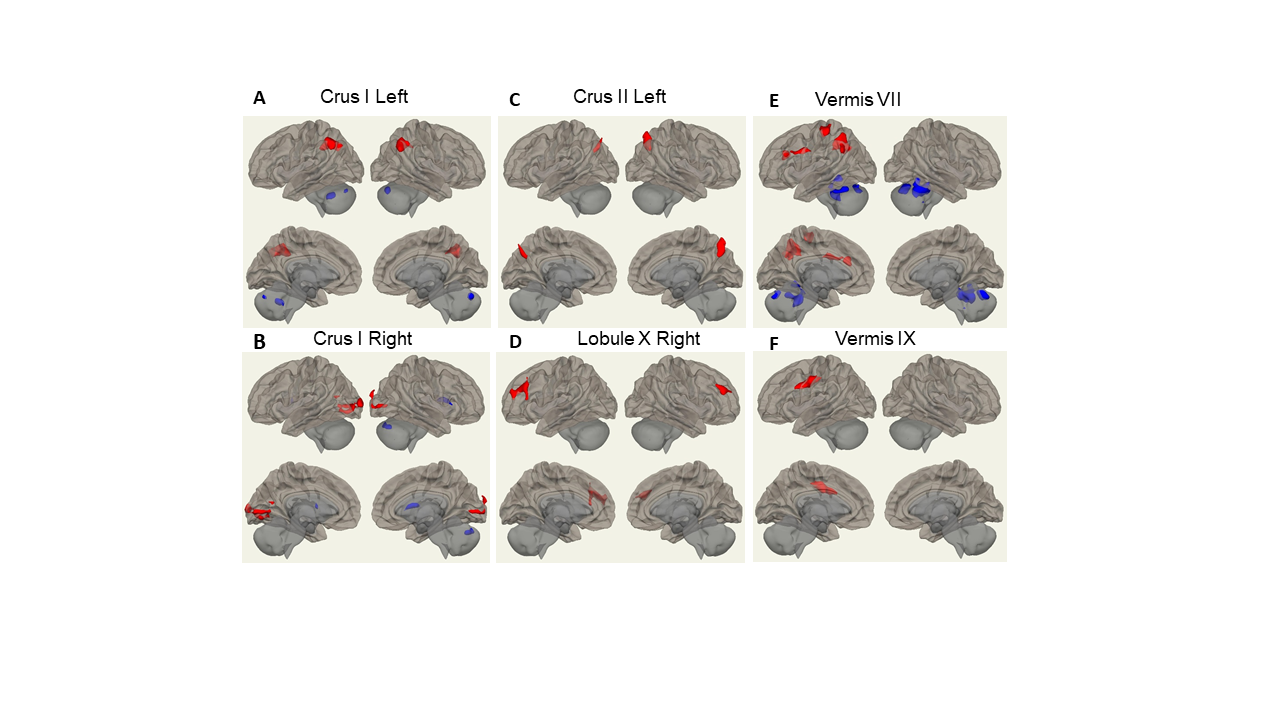
Figure 2: FC difference map between the PD patients and HCs of non-motor cerebellum seeds of (A) left Crus I; (B) right Crus I; © left Crus II; (D) right Lobule X; (E) vermis VII; (F) Vermis IX. Two-sided two sample t-test was performed with significant level of voxel uncorrected p < 0.005 and cluster FDR-corrected p < 0.05. Blue color represents FC of PD less than FC of HCs. Red color represents FC of PD greater than FC of HCs.
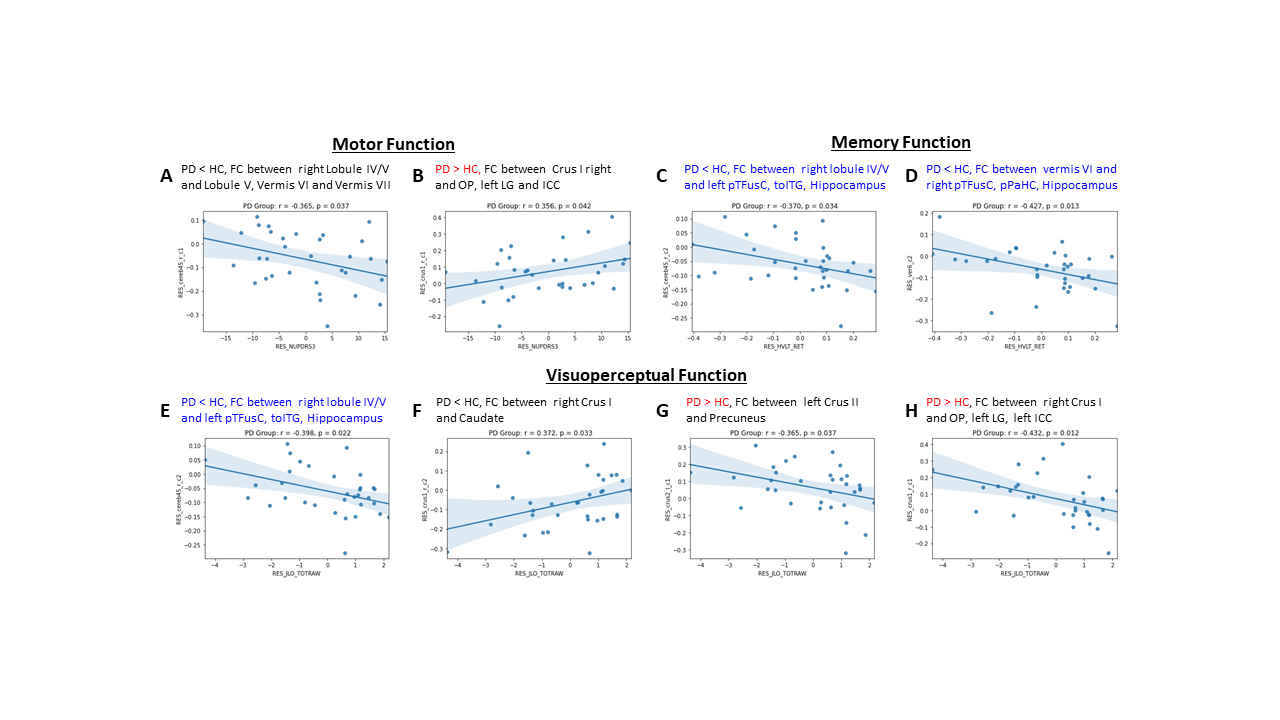
Figure
3:
Association between FC within significant clusters and neurophysiological
assessments in PD group. Correlation between UPDRS III and FC
of (A) right lobule IV/V FC to lobule V, vermis VI, and vermis VII; (B)
right Crus I to OP, left LG, ICC. Correlation between HVLT retention
and FC of (C) right lobule IV/V FC to left pTFusC,
left toITG, and
hippocampus; (D)
vermis VI to right pTFusC, left toITG, and
hippocampus. Correlation between BJLO total raw score and FC of (E) right
lobule IV/V to left pTFusC, toITG, and
Hippocampus; (F) right Crus I to caudate; (G)
left Crus II to Precuneus.
