1Radiology, Fujita Health University School of Medicine, Toyoake, Japan, 2Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University School of Medicine, Toyoake, Japan, 3Division of Functional and Diagnostic Imaging Research, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 4Canon Medical Systems Corporation, Otawara, Japan, 5Diagnostic Radiology, Hyogo Cancer Center, Akashi, Japan
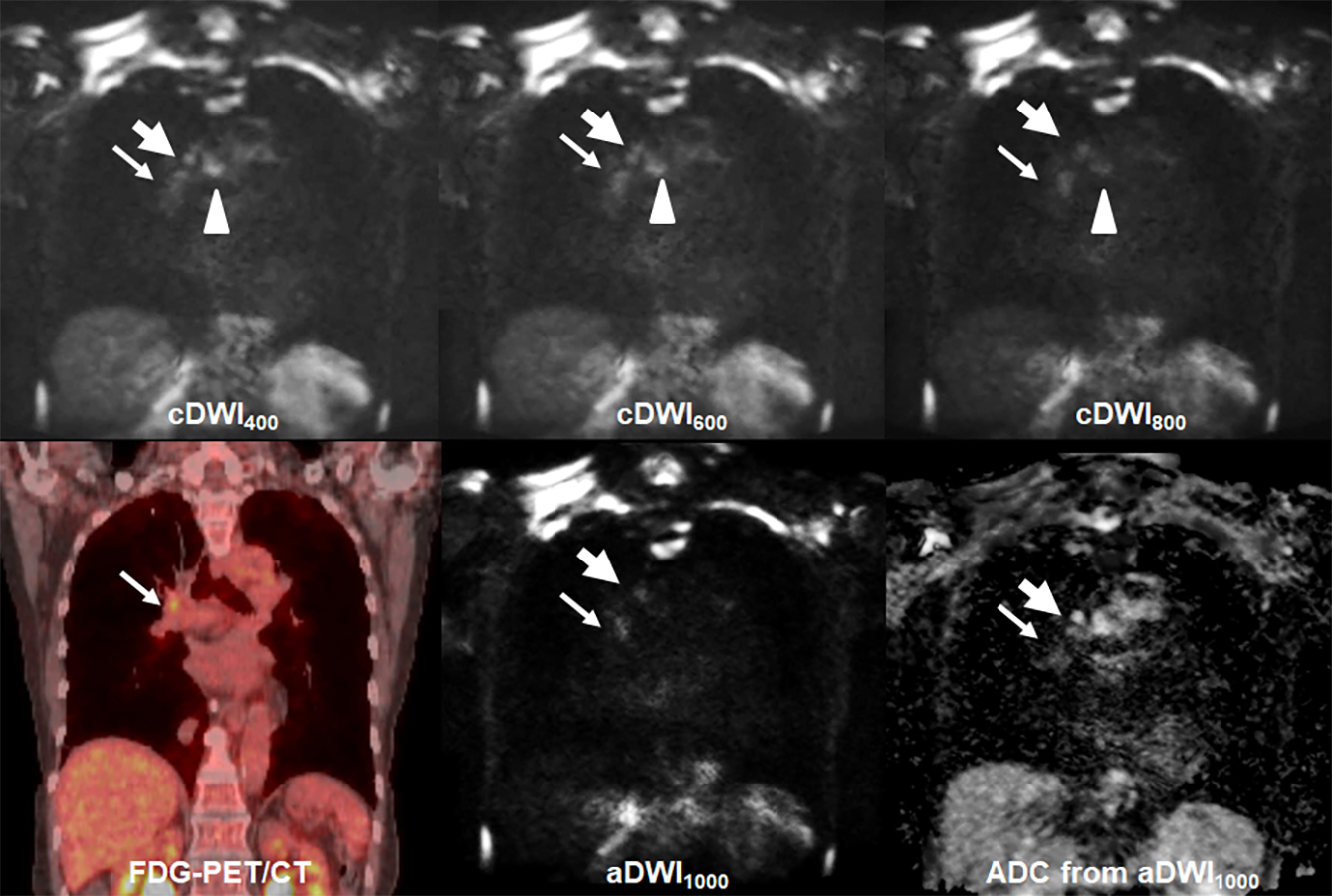
Figure 1. 72-year old invasive adenocarcinoma with N2 disease
cDWI at each b value demonstrates right hilar, right lower paratracheal, subcarina lymph node metastases (arrow, large arrow and arrow head). However, PET/CT shows only right hilar lymph node metastasis (arrow). On the other hand, aDWI and ADC demonstrate right hilar and right lower paratracheal lymph node metastases (arrow and large arrow). This case was assessed as N2 case on each cDWI and aDWI and considered as true-positive. However, this case was evaluated as N1 case on PET/CT and considered as false-negative case.

Figure 2. Result of ROC analysis for distinguishing metastatic from non-metastatic lymph nodes.
Area under the curve (AUC) of CR600 (AUC=0.87) was significantly larger than that of SUVmax (AUC=0.77, p=0.003), CR400 (AUC=0.79, p<0.0001) and CR800 (AUC=0.81, p<0.0001). In addition, AUC of CR800 was also significantly larger than that of CR400 (p=0.02).
