Jaume Coll-Font1,2,3, Shi Chen1, Robert A Eder1, and Christopher T. Nguyen1,2,3
1Cardiovascular Research Center, Cardiology Division, Massachusetts General Hospital, Charlestown, MA, United States, 2Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA, United States, 3Harvard Medical School, Boston, MA, United States
1Cardiovascular Research Center, Cardiology Division, Massachusetts General Hospital, Charlestown, MA, United States, 2Athinoula A. Martinos Center for Biomedical Imaging, Charlestown, MA, United States, 3Harvard Medical School, Boston, MA, United States
We evaluated the differences in gradient direction acquisition schemes for whole-heart cardiac DTI and demonstrated that acquiring DW images along different gradient directions is marginally preferable to acquiring multiple repetitions of the same directions.
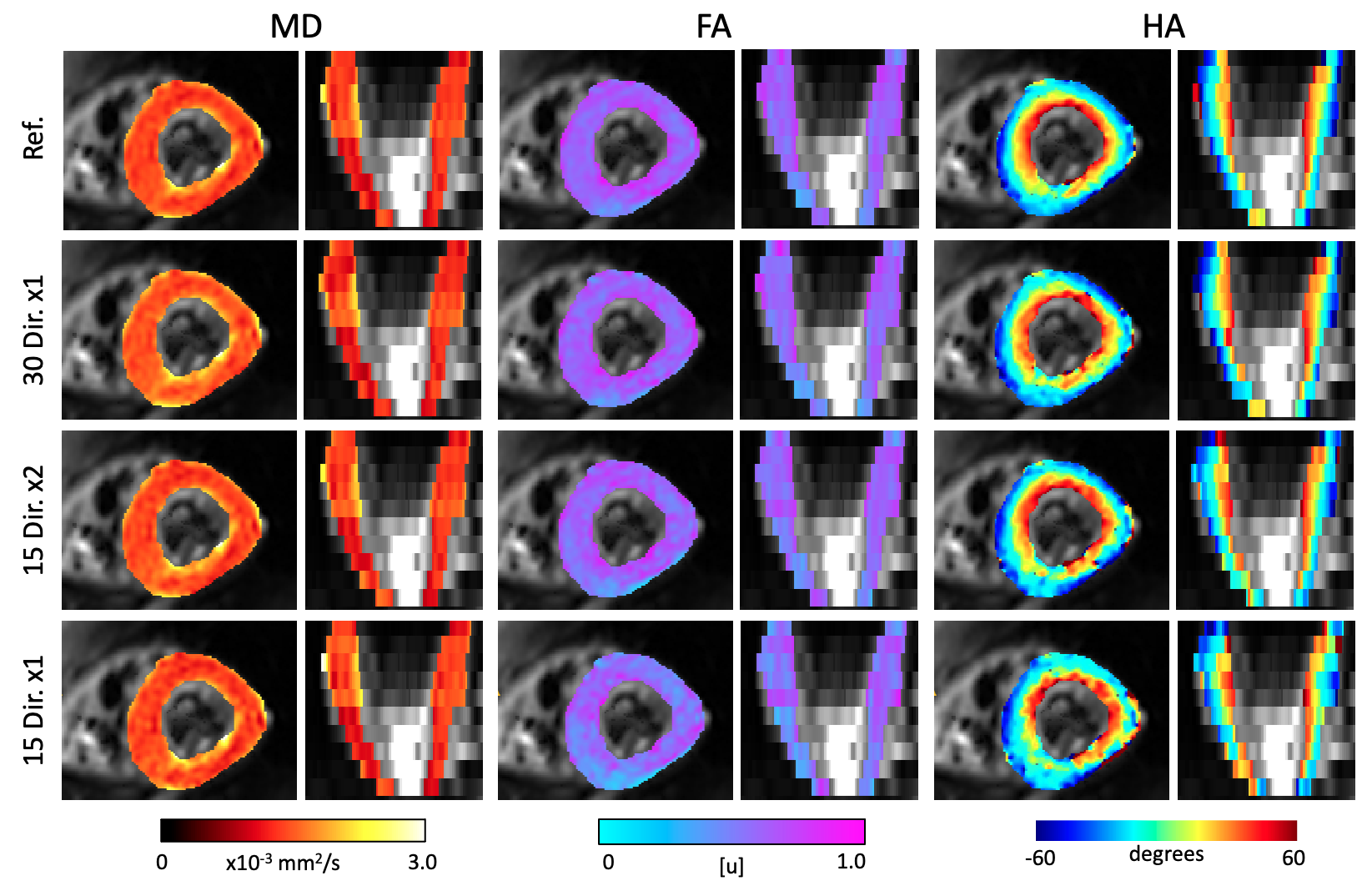
Figure 1. Parameter maps of a representative subject obtained for the different combination of gradient orientations. The rows correspond to the results for all acquired gradient directions (reference: 30 dir. x2), 30x1, 15x2 and 15x1 directions. The maps obtained with at least 30 samples resulted were similar. On the other hand, the DTI fits on only 15 directions resulted in overestimation of FA and disrupted HA maps.
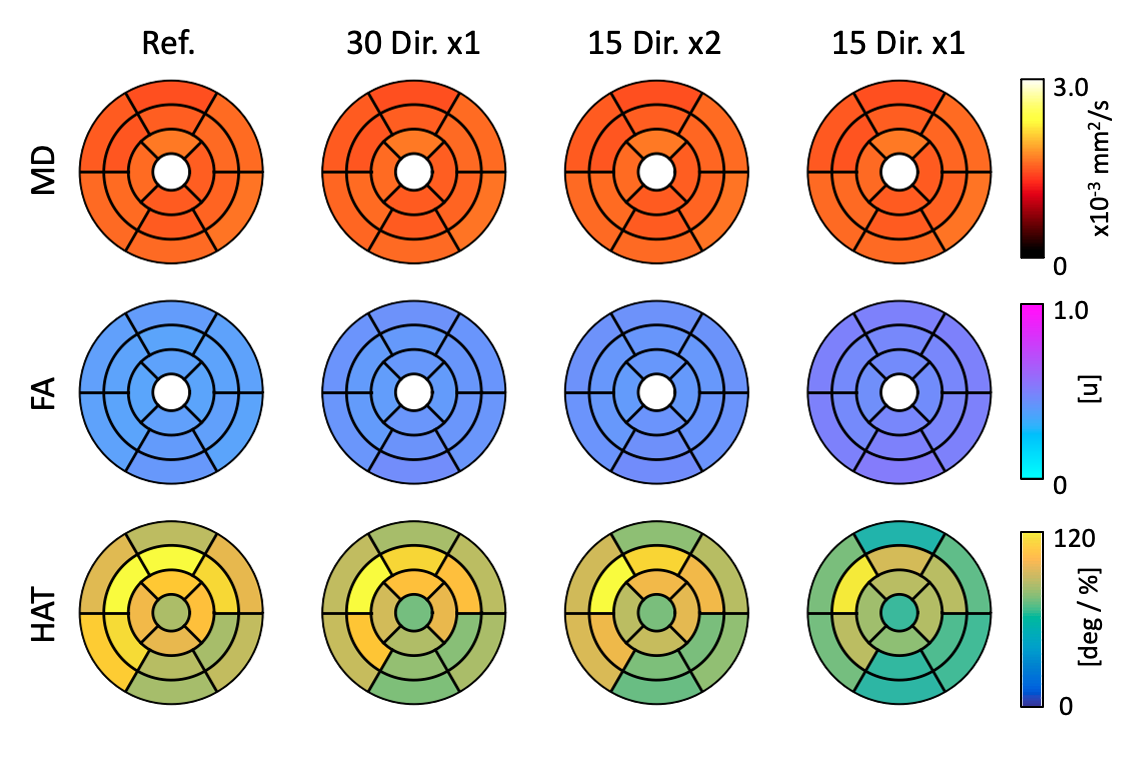
Figure 2. DTI parameters projected on the AHA segments and averaged for all subjects. MD and FA are most robust to different gradient direction selection approaches. On the other, FA and HAT are sensitive to a reduction in the number of samples, as can be observed in the differences of the results obtained with 15 Dir. x1.