Eva van Grinsven1, Anouk Smits1, Emma van Kessel1, Mathijs Raemaekers1, Edward de Haan2, Irene Huenges Wajer1,3, Veerle Ruijters1, Marielle Philippens4, Joost Verhoeff4, Pierre Robe1, Tom Snijders1, and Martine van Zandvoort1,3
1Department of Neurology & Neurosurgery, University Medical Center Utrecht Brain Center, Utrecht University, Utrecht, Netherlands, 2Department of Psychology, University of Amsterdam, Amsterdam, Netherlands, 3Department of Experimental Psychology and Helmholtz Institute, Utrecht University, Utrecht, Netherlands, 4Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands
1Department of Neurology & Neurosurgery, University Medical Center Utrecht Brain Center, Utrecht University, Utrecht, Netherlands, 2Department of Psychology, University of Amsterdam, Amsterdam, Netherlands, 3Department of Experimental Psychology and Helmholtz Institute, Utrecht University, Utrecht, Netherlands, 4Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands
Despite several
differences in the lesion-symptom maps when comparing a tumor and stroke
population, our preliminary conclusion is that these two populations can
provide complementary information regarding involvement of brain regions for
given cognitive tasks.
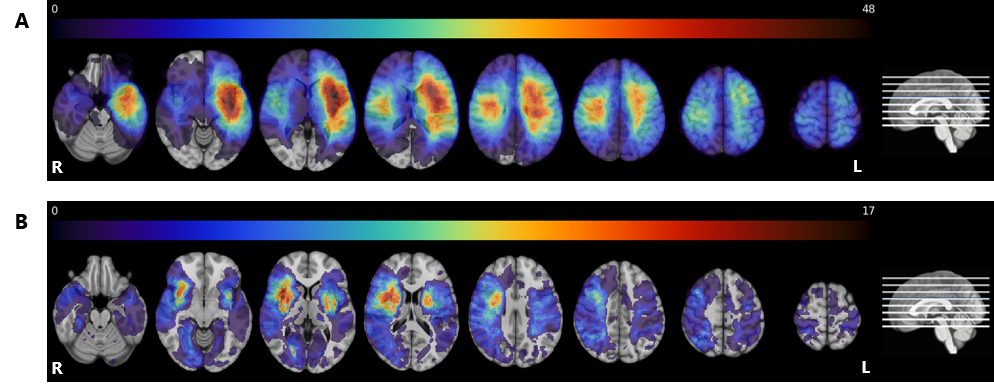
Lesion
prevalence maps for the tumor (panel A) and stroke group (panel B) are shown
superimposed on the MNI brain in radiological view. The colors refer to the
number of patients with a lesion at that voxel, with red indicating a higher
number of patients. The maximum overlap is 48 and 17 for the tumor and stroke
group, respectively. The MNI brain on the right indicates the location of the
slices shown in the figure.
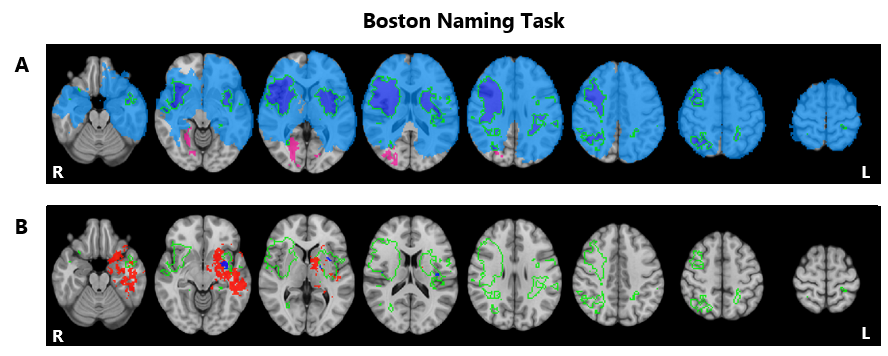
Lesion
symptom results for the Boston Naming Task. Lesion overlap indicating those
regions in which at least 3 patients had a lesion for the tumor group in blue (N=172),
the stroke group in pink (N=103), and overlapping regions shown in the green
outlined purple area (Panel A). Voxels significantly associated with
performance on this task for the tumor group (red) and stroke group (blue) with
the green outline indicating overlapping lesion coverage, as shown in the above
panel (Panel B). Maps are shown on the MNI standard brain in radiological view.
